
The Shoulder
How Does the Shoulder Work?
How Does the Shoulder Work?

The shoulder provides the greatest freedom of movement of any joint in the human body. The glenohumeral joint relies heavily on soft-tissue structures surrounding the bony anatomy to maintain stability and promote function. Here, we explain two fundamental concepts of shoulder biomechanics. Understanding them can help patients with certain shoulder pathologies understand why their shoulder may not be functioning as they are accustomed to.
Concavity-Compression
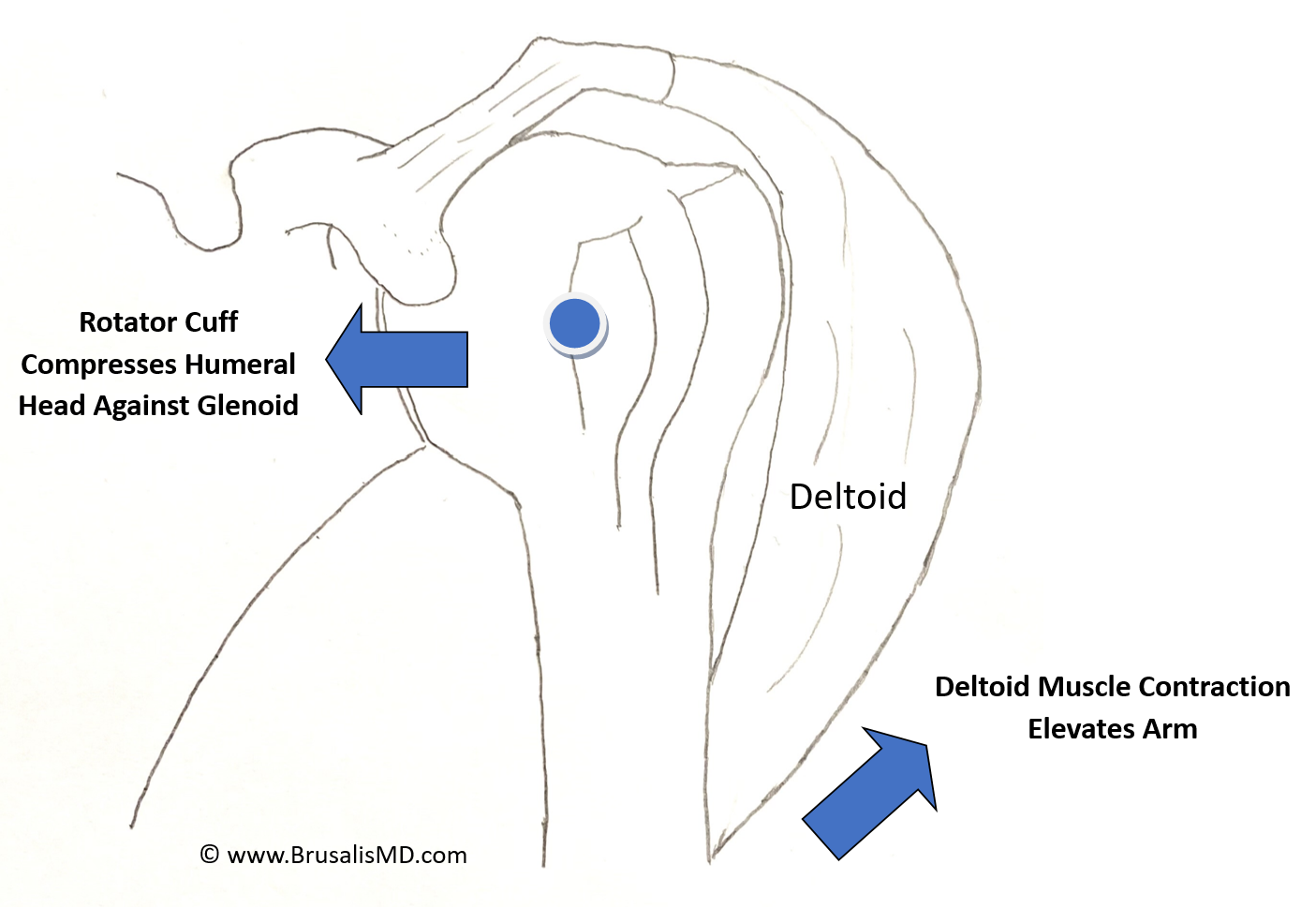
A critical action of the four rotator cuff tendons is to compress the humeral head (ball) against the glenoid (a concave socket). Active contraction of the rotator cuff muscles accomplishes this task, which provides two benefits. First, this confers “dynamic stability,” making it much more difficult for the shoulder to dislocate. For this reason, following a shoulder dislocation or surgery to prevent recurrent dislocations, strengthening of the rotator cuff musculature is a critical part of the rehabilitation process to re-establish these protective forces. Second, active compression by the rotator cuff enables the humeral head to serve as a fulcrum for the deltoid to rotate the arm into abduction. Without a functioning rotator cuff, the humeral head doesn’t hold its position against the glenoid, but instead is pulled superiorly by contraction of the deltoid. Without establishing the humeral head as a stable fulcrum, patients are unable to raise their arm, a condition called “pseudoparalysis.”
Figure 1. A functioning rotator cuff holds the humeral head (ball) against the glenoid (socket). This allows the deltoid to rotate the arm with the center of the humeral head serving as a pivot point, or fulcrum. When the rotator cuff does not work properly, it impairs the ability for a patient to elevate their arm.
Force Couple
A force couple refers to two or more muscles on opposite sides of a joint that work in tandem to maintain stability. The posterosuperior rotator cuff tendons (infraspinatus, teres minor) work as a force couple with the anterior rotator cuff tendon (subscapularis) to help keep the humeral head centered on the glenoid. An imbalance between these muscle groups, either through deconditioning or a tendon tear, can lead to de-centering of the humeral head on the glenoid, increased forces across the glenohumeral joint, and impaired ability to form a stable fulcrum for the deltoid muscle.
Figure 2. A “top-down” view of the left shoulder demonstrates how one rotator cuff muscle in the front of the shoulder (subscapularis) works in tandem with a rotator cuff muscle in the back of the shoulder (infraspinatus) to compress the humeral head (ball) against the glenoid (socket).

Disclaimer: The information provided on this website is intended for informational and educational purposes only. The opinions, views, and content presented here should not be construed as medical advice, diagnosis, or treatment. We welcome you to schedule a consultation with Dr. Brusalis for evaluation of your specific medical condition.